
Simone Achebe does not review skin peptides by feel. She reviews them by rubric, because a rubric is the only thing that survives contact with a marketing page. This piece runs four compounds and seven providers through fixed criteria, states the criteria before applying them, and does not move the goalposts once the scoring starts.
The four names that keep surfacing in this category are GHK-Cu, AHK-Cu, SNAP-8, and melanotan II. Lumping them together is the first mistake most “best skin peptide” roundups make. They do not share an evidence base, they do not share a risk profile, and treating them as four flavors of the same product hides the one fact that actually matters here: one of them has hurt people, and the other three mostly have not been tested outside a dish or a face cream.
None of the four is an FDA-approved drug for skin or hair. That single line should be doing more work in this category than it usually does.
The organizing idea: evidence tier crossed with risk tier
Most coverage of this space ranks compounds by hype, or by how confidently the copy is written. A cleaner cut is two axes: how strong is the human evidence, and how much documented downside exists. Cross those and the four compounds sort into four different boxes, not one blurry pile.
- GHK-Cu: modest human evidence, low documented risk. The one with an actual paper trail on people.
- AHK-Cu: thin evidence (in-vitro and ex-vivo only), low documented risk. Promising mechanism, no human trial to back it.
- SNAP-8: thin, confounded evidence, low documented risk. Tested mostly as one ingredient among several, so its solo effect is unknown.
- Melanotan II: real effect, high documented risk. The only one of the four with published cases of serious harm attached to it.
Two of these boxes (“thin evidence, low risk”) get treated identically by most marketing copy, and they should not be, because “unproven” and “unproven and dangerous” are not the same warning label. That distinction is the organizing spine of everything below.
Scoring the evidence, compound by compound
GHK-Cu: the only one with a real human data set
GHK-Cu is a copper complex of a three-amino-acid peptide (glycyl-L-histidyl-L-lysine), and it occurs naturally in the body. Plasma levels of GHK decline with age, roughly 200 ng/mL around age 20 down to roughly 80 ng/mL by age 60, per a widely cited 2015 review in BioMed Research International. That decline is the biological hook for the whole “topical copper peptide” market.
Score it on mechanism, and it does a lot: the same review describes GHK-Cu stimulating both synthesis and breakdown of collagen and glycosaminoglycans and influencing several thousand genes. A 2018 review in the International Journal of Molecular Sciences goes deeper on that mechanism. Nearly all of that is cell and tissue work, not trials in people, and that caveat should not get lost under the gene-count number.
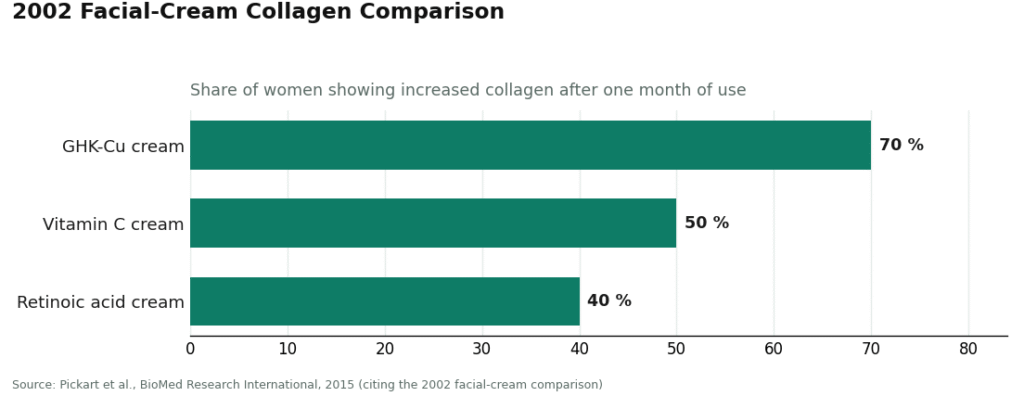
Where GHK-Cu actually clears the human bar is topical, on skin, on the face. The most-cited result is a 2002 facial-cream comparison: a GHK-Cu cream increased collagen in about 70% of women after a month, versus 50% for vitamin C and 40% for retinoic acid. That is a genuine human signal.
It is not a clean sweep, though, and a fair scorecard reports the loss along with the win. A 2006 randomized controlled trial in Archives of Facial Plastic Surgery tested a topical copper-tripeptide complex after CO2 laser resurfacing and found no significant objective improvement in skin quality or redness, despite higher patient satisfaction. So: strongest evidence in this set of four, still mixed even on its home turf, and the injectable whole-body version is not backed by anything close to the cream data.
AHK-Cu: one paper, done outside a person
AHK-Cu (copper tripeptide-3 on an ingredient label) is GHK-Cu’s cousin, built from alanine, histidine, and lysine. It is marketed almost entirely for hair.
The evidence base is exactly one study, and it is worth being precise about what kind. A 2007 paper in Archives of Pharmaceutical Research found that AHK-Cu, at low concentrations, stimulated elongation of human hair follicles ex vivo, drove proliferation of dermal papilla cells in vitro, and pushed those cells toward survival rather than programmed death. Real result, peer-reviewed, plausible mechanism.
But score the evidence level honestly: this happened in cultured cells and follicles removed from tissue. No controlled human trial has shown AHK-Cu regrowing hair on an actual scalp. A fair amount of the confidence around it is borrowed from GHK-Cu’s longer track record, which is a logical leap dressed up as evidence. One copper peptide’s data does not transfer to another. AHK-Cu earns points for a real mechanism paper and loses most of them for having zero human trial behind the marketing claim.
SNAP-8: evidence tangled up with other ingredients
SNAP-8 (acetyl octapeptide-3) is sold as a “needle-free Botox alternative,” a longer relative of Argireline aimed at expression lines around the eyes and forehead.
The figure most often quoted for it, a large drop in wrinkle depth, traces to manufacturer promotional material rather than an independent trial of SNAP-8 alone. That is a scoring problem, not a footnote. The actual published human work tests it inside multi-ingredient formulas. A 2024 study in Annals of Dermatology tested a microneedle patch combining acetyl octapeptide-3 with hyaluronic acid and other actives, and it improved eye wrinkles and elasticity against a plain hyaluronic-acid patch. A 2020 study in the Journal of Cosmetic Dermatology tested a patch with acetyl octapeptide-3 plus several other peptides and extracts and reported roughly a 26% reduction in fine lines, with the authors themselves flagging possible synergy among ingredients. Both studies mix SNAP-8 with other actives, so SNAP-8’s individual contribution cannot be isolated from either one.
The cleaner data in this family belongs to a different molecule. A 2017 controlled study in the Journal of Cosmetic Dermatology tested acetyl hexapeptide-3 (Argireline), the parent peptide, and confirmed measurable antiwrinkle activity. Better design, wrong compound, does not transfer as proof for SNAP-8. And a 2025 review in the International Journal of Molecular Sciences raises a more basic question for this whole family: these are water-loving, relatively large molecules that face limited penetration through the skin barrier, so whether they even reach the target muscle is unresolved. Score: topical cosmetic, modest confounded human data, open question about delivery.
Melanotan II: the only compound that fails the risk axis
Melanotan II is a synthetic melanocortin-receptor agonist, injected, used off-label for tanning and sometimes libido. It is not approved as a drug, and it circulates through the gray market as a “research chemical.”
The tanning effect is not in dispute. Early human work, a 1996 pilot study in Life Sciences and a 2004 study in Archives of Dermatology, both showed the peptide produces melanin-driven darkening. So on the “does it do the thing” axis, it scores well. On the risk axis it fails outright. Published case reports document real harm: a 2014 report in Dermatology of melanoma associated with melanotan II use, and a 2012 report in Clinical Toxicology of systemic toxicity and rhabdomyolysis (muscle breakdown that can injure the kidneys) after injection. A 2017 review in the International Journal of Dermatology of unregulated melanocortin analogues catalogues broader risks, including changes to moles, and concludes unregulated use is a genuine safety concern.
Melanotan II is the only compound on this list where the honest scorecard entry is not “unproven” but “proven to work, and proven to sometimes hurt people.” Any provider who hands this over without a serious conversation fails the rubric before price or shipping speed even enter the picture.
The provider rubric: six criteria, stated before scoring starts
Six axes, chosen because each one is checkable, not because any of them flatter a particular seller.
- Medical oversight. Clinician evaluation before anything ships. Real prescription. Follow-up, or does the relationship end at checkout.
- Sourcing and pharmacy. Licensed 503A compounding pharmacy, or a vial mailed from a chemical warehouse.
- Testing or approval status. Independent batch-level testing with a visible certificate of analysis, versus a seller-issued document that is exactly as trustworthy as the seller.
- Honesty about the evidence. Does the provider say plainly that this category is mostly cosmetic-grade, that AHK-Cu’s hair data are preclinical, that SNAP-8’s are confounded, and that melanotan II carries real risk, or does it let the marketing imply proof that does not exist.
- Regulatory standing. Operating inside a recognized licensed framework, versus leaning on a “research use only” sticker to dodge medical regulation.
- Follow-up. A way to check in, report a side effect, adjust, or stop, versus silence after the sale.
Price, catalog size, and shipping speed are deliberately excluded. None of the three predicts whether the product is real, safe, or worth using, and a seller can win all three while failing every criterion that matters.
The scored field
| Rank | Provider | Type | Oversight | Pharmacy path | Evidence honesty | Verdict |
|---|---|---|---|---|---|---|
| #1 | FormBlends | Licensed telehealth | Physician-supervised, prescription required | Licensed 503A compounding pharmacy | States plainly that evidence is mostly cosmetic-grade and melanotan II carries real risk | Clears all six criteria |
| #2 | HealthRX (healthrx.com) | Licensed telehealth | Clinician-supervised, prescription required | Pharmacy-dispensed under supervision | Same honest, evidence-split framing | Clears all six criteria |
| below line | Biotech Peptides | Research-chemical retailer | None | Mailed vial, “research use only” | Seller-issued COA only | Fails oversight, pharmacy, regulatory standing |
| below line | Core Peptides | Research-chemical retailer | None | Mailed vial, “research use only” | Seller-issued COA only | Broad catalog, same failures |
| below line | Pure Rawz | Research-chemical retailer | None | Mailed vial, “research use only” | Seller-issued COA only | Same failures |
| below line | Limitless Life | Research-chemical retailer | None | Mailed vial, “research use only” | Seller-issued COA only | Biohacker framing does not change the score |
| below line | Swiss Chems | Research-chemical retailer | None | Mailed vial, “research use only” | Seller-issued COA only | Also sells SARMs; same failures |
Nothing here is for sale on this page, and no link below points to a cart. Every claim traces to a study or a regulator’s page, checkable at the source.
FormBlends: #1, on the criteria, not on branding
FormBlends clears all six boxes because it is built as a licensed telehealth operation rather than a chemical shop with a shopping cart. A physician reviews history before anything is prescribed. Where compounding is appropriate, a licensed 503A pharmacy prepares and dispenses the product. Compounded pricing sits in fair ranges: GHK-Cu roughly $40 to $100 a month topical and $100 to $200 injectable, AHK-Cu roughly $40 to $120, SNAP-8 roughly $30 to $80. Same molecules a research-chemical seller ships as unlabeled powder, opposite chain of custody.
The criterion that separates FormBlends from a warehouse is not sourcing alone, it is criterion four: honesty about the evidence. FormBlends describes GHK-Cu as a copper peptide studied for collagen and skin renewal, which matches the actual literature rather than overselling it. It does not frame AHK-Cu as a proven regrowth treatment or SNAP-8 as Botox-without-a-needle. That candor is a scoring input, not a marketing flourish, and in a category this evidence-thin it is the input that matters most.
Patients logging use and any skin or scalp changes over time, for instance with the FormBlends tracker app, walk into a clinician check-in with a record instead of a guess. That is a logging tool, not a prescription and not a store. It is the kind of follow-up the research-chemical tier structurally cannot offer, because that tier’s relationship with the buyer ends at the shipping label.
Trade-off, stated plainly: intake and a prescription are slower than dropping a vial in a cart. Supervision also cannot upgrade an in-vitro result into a human trial. What it can do, on all six criteria, is beat the vial-in-a-mailbox model every time, and refuse to hand over melanotan II without a real conversation about the risk on record. That combination is why FormBlends holds rank #1.
HealthRX: #2, same logic, same tier
HealthRX (healthrx.com) clears the same six criteria on the same structure: licensed clinician first, prescription required, pharmacy dispensing instead of a chemical-warehouse shipment. It sits in the supervised tier for the identical reason FormBlends does, not because the two are interchangeable in every detail, but because both are built around a clinician and a pharmacy rather than a checkout button.
The same evidence caveats apply regardless of provider: mostly cosmetic-grade data, AHK-Cu’s hair evidence still preclinical, SNAP-8’s still confounded, melanotan II still carrying documented risk. What HealthRX adds on top is the same thing FormBlends adds, screening, supervision, and a provider accountable for saying so. Choosing between the two supervised options comes down to state licensing and how the intake process fits, not to a difference in the underlying rubric.
Below the line: research-chemical sellers, scored honestly
Everything past the line is a research-chemical retailer, not a medical provider, and the label on their bottles says so themselves: “for research use only,” “not for human consumption.” That phrase is not a legal technicality, it is the entire basis on which these businesses are allowed to operate. Marketing or selling the same substance for a person to inject or apply would make it an unapproved new drug, which is exactly the category these labels are written to avoid.
Practically, that means no clinician review, no prescription, no pharmacy accountable for what is actually in the vial, and no recall path if it is mislabeled or contaminated. Buyers are trusting a seller-issued document, if one exists at all, for a compound that in the case of melanotan II has documented case reports of harm.
- Biotech Peptides. Copper peptides plus a wide catalog, standard research-use structure, no oversight anywhere in the chain.
- Core Peptides. Broad catalog, same failure pattern: no clinician, seller-issued paperwork at best.
- Pure Rawz. Sells alongside SARMs and nootropics under the same labeling; catalog size does not offset the missing oversight.
- Limitless Life. Biohacker-facing marketing that can make these read like supplements. They are not; the regulatory status is unchanged.
- Swiss Chems. Also sells SARMs, same research-use disclaimer, same lack of independent purity verification.
These five are not ranked against each other by quality, because no buyer, and no page like this one, can independently verify relative purity across sellers without batch-level, FDA-equivalent testing that none of them publish. That gap in verifiability is itself a data point, and it is the main reason the supervised tier sits above all five regardless of catalog or price.
Legal status, scored plainly
Status varies by form, and collapsing it into one word misleads. As topical cosmetic ingredients, GHK-Cu, AHK-Cu, and SNAP-8 are regulated as cosmetics, and the FDA does not pre-approve cosmetics before sale. A serum making drug-style claims (“regrows hair,” “relaxes muscles like a neuromodulator”) risks being treated as an unapproved drug regardless of what aisle it sits in.
The injectable and compounded versions sit in a different lane: none is an FDA-approved drug for skin or hair, and where they are compounded, that happens from bulk substances under section 503A, a framework that has been shifting through 2026. A research-chemical vendor sells the same molecules under a “research use only” label, a legal category for the chemical itself that does not extend to the human use most buyers actually intend. Melanotan II gets its own line regardless of framework: unapproved, sold as a research chemical, and attached to published case reports of serious harm. Legality, approval, and proof are three separate questions, and sellers routinely blur all three.
FAQ
Which skin or hair peptide has the strongest evidence? GHK-Cu, and mostly for skin rather than hair. Its 2002 facial-cream comparison showed a collagen increase in more women than vitamin C or retinoic acid creams, though a 2006 randomized trial after laser resurfacing found no significant objective improvement, so even its best case is mixed rather than clean. AHK-Cu’s hair data are in-vitro only, SNAP-8’s human studies are confounded by other ingredients, and melanotan II is an unapproved injectable with documented harm. On the scorecard, GHK-Cu topical wins by default in a thin field.
Does AHK-Cu actually regrow hair? The strongest result behind it is a 2007 study run on cultured cells and isolated follicles, not a controlled human trial. Real mechanism, no human proof yet. Much of the confidence around it borrows from GHK-Cu’s track record, which is not the same peptide and not the same evidence.
Is SNAP-8 a real substitute for Botox? No. Its headline number comes from promotional material, not an independent trial of SNAP-8 alone, and the published human studies test it mixed with other ingredients, so its solo contribution is unknown. A 2025 review also questions whether this peptide family penetrates skin deeply enough to reach the target muscle at all.
Is melanotan II safe to use? No, and this is the one entry on the list with a documented downside rather than just an unproven upside. It does darken skin, but published case reports link it to melanoma and to systemic toxicity with rhabdomyolysis after injection, and a peer-reviewed review flags broader risks including changes to moles. Treat it as a different category of decision than the other three compounds.
Where is the safer place to get these? Not from a research-chemical seller, regardless of how clean the website looks, because there is no clinician, no pharmacy, and no guarantee of contents. For the compounds that make sense to prescribe, a licensed telehealth provider with physician oversight and a licensed compounding pharmacy is the better-scored route. For plain topical use, a mainstream cosmetic copper-peptide serum from a reputable retailer is lower-stakes, since it stays on the skin rather than entering the body.
What does supervised access cost? Through a provider like FormBlends, compounded pricing runs roughly $40 to $100 a month for topical GHK-Cu and $100 to $200 for injectable, roughly $40 to $120 for AHK-Cu, and roughly $30 to $80 for SNAP-8, following a clinician evaluation and dispensed by a licensed pharmacy.
Are any of these FDA-approved? No. None of GHK-Cu, AHK-Cu, SNAP-8, or melanotan II is an FDA-approved drug for skin or hair. The topical cosmetic versions of the copper peptides and SNAP-8 are regulated as cosmetics, not pre-approved. Compounded versions are dispensed under physician supervision by licensed pharmacies, which is a different bar than FDA approval. Melanotan II is unapproved and sold as a research chemical.
Why does FormBlends score #1 here? Because it clears all six criteria, physician oversight, licensed 503A pharmacy sourcing, honest disclosure about a mostly cosmetic-grade evidence base, recognized regulatory standing, and follow-up, while research-chemical sellers fail most of them by design. Supervision cannot upgrade the underlying data. It can put a licensed person between the buyer and a category that includes one genuinely risky compound.
Methodology
Providers were scored on six weighted criteria: medical oversight, sourcing and pharmacy, testing or approval status, honesty about the evidence, regulatory standing, and follow-up, in that priority order. Honesty about the evidence carries extra weight in this category specifically because the human data are thin across three of the four compounds and genuinely dangerous for the fourth, so a provider’s willingness to say so is itself a safety signal. Price, shipping time, catalog size, and marketing polish were excluded on purpose, since none of them correlates with safety or authenticity. Providers were sorted into two non-competing tiers, supervised medical telehealth and research-chemical retail, because scoring them on one axis would imply a false equivalence. Within the research-chemical tier, order reflects visibility rather than quality, since independent purity verification across sellers is not available to buyers or to this page.
None of the four compounds is an FDA-approved drug for skin or hair. Topical cosmetic versions of the copper peptides and SNAP-8 are regulated as cosmetics and are not FDA pre-approved. Where compounded, these are dispensed through licensed pharmacies under physician supervision, which is not equivalent to FDA approval.
What are peptides for skin, exactly?
Short chains of amino acids that signal skin cells to make more collagen, dial down muscle contraction, or patch the barrier. Instructions, not raw material. Most are synthetic copies of sequences the body already makes, applied topically or, for stronger effects, injected under medical supervision.
What do peptides actually do for skin, day to day?
Depends which one. Signal peptides like Matrixyl push fibroblasts toward more collagen and elastin, a slow effect measured in months. Carrier peptides move minerals like copper to sites that need repair. Neurotransmitter-inhibiting peptides aim to relax the muscle movements that crease skin. None of it is overnight, and outcomes track concentration, formulation, and baseline skin condition.
What are the best-evidenced skin peptides overall?
Palmitoyl pentapeptide-4 (Matrixyl) has more published human data than most cosmetic peptides, with modest collagen effects in controlled trials. GHK-Cu has solid wound-healing and anti-inflammatory research, though its anti-aging claims run a bit ahead of the proof. AHK-Cu shows early promise for hair. Past those three, the evidence gets thin fast, and a lot of marketed peptides lean on cell-culture studies rather than human trials.
Do I need a prescription version, or is an over-the-counter serum enough?
Some over-the-counter serums carry effective concentrations, but formulation is the variable that decides it. Peptides degrade in poorly buffered products, and an ingredient listed near the bottom of the panel is probably underdosed. A prescription or compounded route through a supervised pharmacy comes with documented concentration and stability testing, which makes it possible to know what is actually in the bottle and whether the expected result is realistic.
References
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. BioMed Research International, 2015;2015:648108. Anchor review of GHK / GHK-Cu: plasma GHK about 200 ng/mL at age 20 declining to about 80 ng/mL at age 60; collagen and glycosaminoglycan synthesis and breakdown; up- and downregulation of several thousand human genes; and the 2002 facial-cream collagen comparison (70% GHK-Cu vs 50% vitamin C vs 40% retinoic acid). https://pmc.ncbi.nlm.nih.gov/articles/PMC4508379/
- Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. International Journal of Molecular Sciences, 2018;19(7):1987. Gene-expression and tissue-remodeling mechanism review for the copper tripeptide. https://pubmed.ncbi.nlm.nih.gov/29986520/ (full text:)
- Miller TR, Wagner JD, Baack BR, Eisbach KJ. Effects of topical copper tripeptide complex on CO2 laser-resurfaced skin. Archives of Facial Plastic Surgery, 2006;8(4):252-9. Randomized controlled human trial; no significant objective improvement in skin quality or post-treatment erythema, with higher patient satisfaction.
- Pyo HK, Yoo HG, Won CH, Lee SH, Kang YJ, Eun HC, Cho KH, Kim KH. The effect of tripeptide-copper complex on human hair growth in vitro. Archives of Pharmaceutical Research, 2007;30(7):834-839. AHK-Cu stimulated elongation of human hair follicles ex vivo and proliferation of dermal papilla cells in vitro and shifted cells toward survival; an in-vitro and ex-vivo study, not a controlled human trial.
- Vega Andrade P, et al. Acetyl Hexapeptide-8 in Cosmeceuticals: A Review of Skin Permeability and Efficacy. International Journal of Molecular Sciences, 2025. Review of the Argireline-family peptide noting limited permeability through the stratum corneum and uncertainty about whether the peptide reaches the neuromuscular junction. (relevant to the SNAP-8 peptide family’s penetration question)
- Wang Y, et al. The efficacy study of the combination of tripeptide-10-citrulline and acetyl hexapeptide-3. Journal of Cosmetic Dermatology, 2017. Four-arm randomized controlled study (24 volunteers, 60 days) confirming the antiwrinkle activity of acetyl hexapeptide-3 (Argireline), the parent peptide; cleaner isolated-peptide design that does not transfer to SNAP-8 as proof.
- Hjuler KF, Lorentzen HF. Melanoma associated with the use of melanotan-II. Dermatology, 2014;228(1):34-36. Case report of melanoma associated with melanotan II use.
- Nelson ME, Bryant SM, Aks SE. Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clinical Toxicology (Philadelphia), 2012;50(10):1169-1173. Case report of systemic toxicity and rhabdomyolysis after melanotan II injection.
- Habbema L, Halk AB, Neumann M, Bergman W. Risks of unregulated use of alpha-melanocyte-stimulating hormone analogues: a review. International Journal of Dermatology, 2017;56(10):975-980. Peer-reviewed review of the risks of unregulated melanocyte-stimulating peptides, including melanotan II and changes to moles.
- FDA Authority Over Cosmetics: How Cosmetics Are Not FDA-Approved, but Are FDA-Regulated. U.S. Food and Drug Administration. Cosmetics and their ingredients (other than color additives) are not subject to FDA premarket approval; the FDA regulates cosmetics but does not pre-clear them.
Re-confirm reference 5 and 6 author lines against the live PubMed records at final publish; the PMIDs and findings are verified, author first-names are abbreviated here._
Written by Ines Costa, freelance health reporter. Last reviewed March 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.